we are transitioning over to a new website:
dailyem.wordpress.com
update your readers!
New format is a work in progress, so feedback is appreciated. check it out!
Wednesday, June 13, 2012
Friday, June 8, 2012
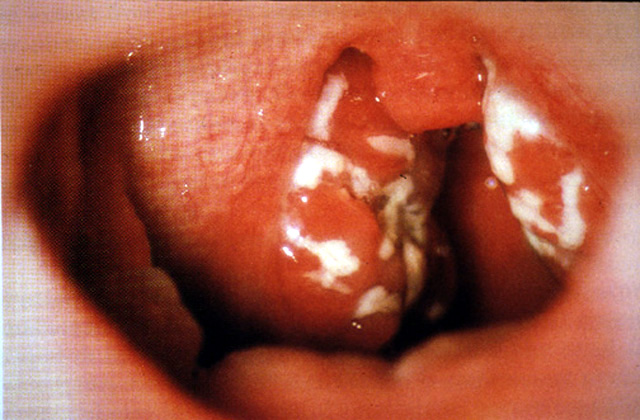
stevens johnson syndrome...without a rash

--severe idiosyncratic reactions, most commonly triggered by medications, which are characterized by fever and mucocutaneous lesions leading to necrosis and sloughing
--less severe disease on the same spectrum as TEN (toxic epidermal necrolysis)
DIAGNOSIS: NOT FAIR
--apparently, you can have Stevens-Johnson syndrome without a rash
PMID: 22041607
The Stevens-Johnson syndrome (SJS) classically involves a rash, conjunctivitis and mucositis.
case report of isolated mucositis and conjunctivitis.
Previous rare reports of severe SJS like syndromes without a rash are confined to children, usually with mycoplasma pnemoniae infection
PMID: 22012144
The commonest infections associated with SJS have been HSV and Mycoplasma pneumoniae.
Less than 10% cases of Mycoplasma pneumonia develop extra pulmonary complications like hemolytic anemia, hepatitis, arthritis, meningitis and SJS.
unclear from existing literature whether antibiotic treatment of M. pneumoniae infection decreases the risk for SJS.
PMID: 20678095
another case report of mucocutaneous involvement without skin lesions.
Oral lesions are present in all cases with SJS associated with M. pneumoniae infection, ocular lesions only in two-thirds and genital lesions in three-fourths of all cases.
That SJS in association with M. pneumoniae infection is predominantly mucosal is reflected by few reports of SJS presenting without skin lesions. Even when skin lesions are present, mucocutaneous lesions predominate.
BOTTOM LINE:
--stevens johnson syndrome: skin and mucosal involvement, can progress to sloughing (e.g. TEN)
--can present withOUT rash. Mycoplasma pneumonia is common source.
Submitted by J. Gullo.
Reference(s): uptodate.com: Stevens-Johnson syndrome and toxic epidermal necrolysis: Clinical manifestations; pathogenesis; and diagnosis; article 1, article 2, article 3; picture
Tuesday, June 5, 2012
when not to use succinylcholine
BLATANT REDIRECT:
 --check out EMCrit's handy slide
--check out EMCrit's handy slide
 --check out EMCrit's handy slide
--check out EMCrit's handy slide
--good quick review of when you can (or can't) use succinylcholine
BOTTOM LINE:
--check out the slide on EMCrit
--if you can't or are lazy, remember succinylcholine causes K+ release
--also, hyperkalemia is bad
--first do no harm
Reference(s): emcrit.org; picture
Monday, June 4, 2012
loop abscess

Looking for a fun and interesting new way to treat an abscess?
(I've done it once, with good success.)
You tube video - only 2 minutes long, worth watching, and worth
reviewing in the ED before actually trying this:
Dr. Tsoriades and colleagues found using a vessel loop (see picture)
was a safe and effective treatment for subcutaneous abscesses in children when
studied in comparison with traditional incision and drainage with packing.
Children in the study were under general anesthesia or conscious
sedation. (I used a traditional field block using 2% lidocaine with epinephrine
in an adult.)
Pros:
- no repeat packing
- better tolerated by patients
- less wound care materials
- much smaller incision - less scarring
Discharge instructions:
- apply warm compresses
- expect drainage
- move loop back and forth 2 times daily
- return if worse/fever/increasing redness
Submitted by S. Morris.
{kind=link}
Friday, June 1, 2012
laws of the house of god
 from THE HOUSE OF GOD, by Samuel Shem, M.D.
from THE HOUSE OF GOD, by Samuel Shem, M.D.--haven't read this in a few years, but came upon this list again recently.
--my favorites are #'s 3 & 6.
--enjoy
- GOMERS DON’T DIE.
- GOMERS GO TO GROUND.
- AT A CARDIAC ARREST, THE FIRST PROCEDURE IS TO TAKE YOUR OWN PULSE.
- THE PATIENT IS THE ONE WITH THE DISEASE.
- PLACEMENT COMES FIRST.
- THERE IS NO BODY CAVITY THAT CANNOT BE REACHED WITH A #14G NEEDLE AND A GOOD STRONG ARM.
- AGE + BUN = LASIX DOSE.
- THEY CAN ALWAYS HURT YOU MORE.
- THE ONLY GOOD ADMISSION IS A DEAD ADMISSION.
- IF YOU DON’T TAKE A TEMPERATURE, YOU CAN’T FIND A FEVER.
- SHOW ME A BMS (Best Medical Student, a student at the Best Medical School) WHO ONLY TRIPLES MY WORK AND I WILL KISS HIS FEET.
- IF THE RADIOLOGY RESIDENT AND THE MEDICAL STUDENT BOTH SEE A LESION ON THE CHEST X-RAY, THERE CAN BE NO LESION THERE.
- THE DELIVERY OF GOOD MEDICAL CARE IS TO DO AS MUCH NOTHING AS POSSIBLE.
Reference(s): thanks, dr. wikipedia; picture
Thursday, May 31, 2012
Antibiotics for MRSA abscesses? NO.
STUDY #1:

Schmitz et al. Randomized Controlled Trial of
Trimethoprim-Sulfamethoxazole for Uncomplicated Skin Abscesses in Patients at
Risk for Community-Associated Methicillin-Resistant Staphylococcus aureus
Infection. Annals of Emergency Medicine, Vol 56, Sept 2010
Bactrim vs. placebo after incision and drainage.
Multicenter, double-blind, RCT in 4 military ED's
outcome: treatment failure after 7 days or reduction of new lesion
formation in 30 days
results:
Tx failure 7 days New lesion
within 30 days
Placebo 26%
28%
TMP/SMX 17%
9%
Difference (95%CI) 9% (-2 to 21%) 19%
(4-34%)
As shown above, there was a significant difference of new lesions in
30 days. only 45% were available at 30 days. big confidence intervals.
STUDY #2
Duong et al. Randomized, Controlled Trial of Antibiotics
in the Management of Community-Acquired Skin Abscesses in the Pediatric Patient.
Annals of Emergency Medicine, Vol 55, May 2010
Bactrim vs. placebo after incision and drainage.
double-bind RCT in pediatric patients
outcome: treatment failure within 10 days (need for second incision,
IV antibiotics, continued erythema, warmth, fluctuance at 10 day follow up).
results:
Failure to improve 10 day new lesions 90 day new
lesions**
Placebo 5.3% 26.4% 28.8%
TMP/SMX 4.1% 12.9% 28.3%
Placebo 5.3% 26.4% 28.8%
TMP/SMX 4.1% 12.9% 28.3%
** Note that only around 60% were effectively followed up at 90
days.
Conclusion: no difference in failure rates with or without
antibiotics.
Of note, in treatment arm, only 46% of patients were compliant with
antibiotics, taking at least half of the pills.
Note that there are many other studies showing that antibiotic use
does NOT eradicate MRSA.
BOTTOM LINE:
Immunocompetent patients with MRSA abscesses can be treated with I
& D alone. Not enough data to support consistent antibiotic use.
Consider addition of antibiotics in diabetics, immunocompromised,
or systemically ill.
Submitted by S. Morris.
Wednesday, May 30, 2012
passive preoxygenation - a radical concept
 Next time you intubate someone...
Next time you intubate someone...
consider putting them on a nasal
cannula at 15L per min under the NRB.
this article advocates it as a form of "apneic oxygenation"
which can prevent desaturation during intubation.
Awake patients will not
tolerate it at 15L/min, so you can start with 4-5 L and then increase to 15
after giving your induction and paralytic medications.
The point: Apneic oxygenation can extend the duration of safe
apnea.
Note: High O2 could decrease the respiratory drive, but this is for
people who you are committed to intubating already.
I would love to hear your
success stories with this new method!
Submitted by S. Morris.
Reference(s): Weingart, S., Levitan, R. Preoxygenation and Prevention of Desaturation During Emergency Airway Management. Annals of Emergency Medicine. Nov 2011. Vol 9. Iss 3. ; picture
Tuesday, May 29, 2012
steroids for pharyngitis + Centor criteria refresher
STUDY HIGHLIGHTS:
Meta-analysis of 9 RCT's of adults and children using steroids for
tonsillitis or pharyngitis
did find more patients with resolution of pain with
steroids at 24 or 48 hours.
All patients received antibiotics, which may have been
confounding.
BOTTOM LINE:
consider steroids (maybe prednisone 60mg x1 or 2 days)
for adult patients with severe exudative sore throat in conjunction with
antibiotics.
Of course, steroids have complications, so consider them when
prescribing.
Hayward, G. et.al. (2009). Corticosteroids for pain relief in sore throat:
systematic review and meta-analysis. British Medical Journal.
-----
P.S.
a reminder of the Centor criteria (if you believe in them)
The 4 criteria are:
- fever
- pharyngeal exudates
- anterior cervical adenopathy
- absence of a cough.
The presence of a cough, hoarse voice, or
conjunctivitis, suggests a viral etiology and is not considered a risk factor
for group A beta-hemolytic strep.
Centor criteria should not be used to predict
GABS in children.
- <2 points — No antibiotic or throat culture necessary.
(Risk of strep infection <10%) - 2-3 points — Should receive a throat culture and treat with an antibiotic if culture is positive.
- >3 points — Treat empirically with an antibiotic.
(Risk of strep infection >50%)
Singer JI, Gebhart ME: Sore throat, in Marx JA, Hockberger RS, Walls
RM (eds): Rosen's Emergency Medicine Concepts and Clinical Practice, ed 6, St.
Louis: Mosby, 2006: 274
Submitted by S. Morris.
Reference(s): hayward study; rosen's chapter (listed above); picture
Monday, May 28, 2012
broaden your horizons (a.k.a. good luck diagnosing this one in the ED): EE

--patient with esophageal foreign body, mobilizing for GI swallow/scope
--foreign body resolved by the time GI swallow is done
--GI consult requests IgE... why?
Eosinophilic Esophagitis (EE)
--mimics GERD and may result in narrowing or stricture of the esophagus.
--differentiated from GERD by the amount of mucosal eosinophilia and lack of response to acid suppression.
--In a cohort, 71% percent of patients with EE were male with a mean age of 10.5+/-5.4 years.
--strong familial pattern
--sometimes first presents with lodged food boluses 2/2 stricture.
Submitted by T. Boyd.
Reference(s): Noel et al. Eosinophilic Esophagitis Correspondence. NEJM. 351:940-941. Aug 2004. picture
Thursday, May 24, 2012
broaden your horizons (a.k.a. good luck diagnosing this one in the ED): HLH

--a condition where there is uncontrolled activation of the cellular immune system.
--Diagnostic criteria include:
- idiopathic fever
- spleenomegaly
- cytopenias
- hypertriglyceridemia
- hypofibrinogenemia
- lymphadenopathy
- rash
- presence of hemophagaocytosis
- erythroderma
- generalized purpuric macules and papules
- morbilliform eruptions.
--Basically this is a rare but potentially fatal disease that no Emergency Physician will ever diagnose.
--BUT if a patient comes in with this in their medical history, now you (sort of) know what to expect
Submitted by T. Boyd.
Reference(s): Favara BE. Hemophagocytic Lymphohistiocytosis: A He mophagocytic Syndrome. Smnr Diag Path. 1992. Schwartz et al. Lymphohistiocytosis. Emedicine. May 2011, picture
Wednesday, May 23, 2012
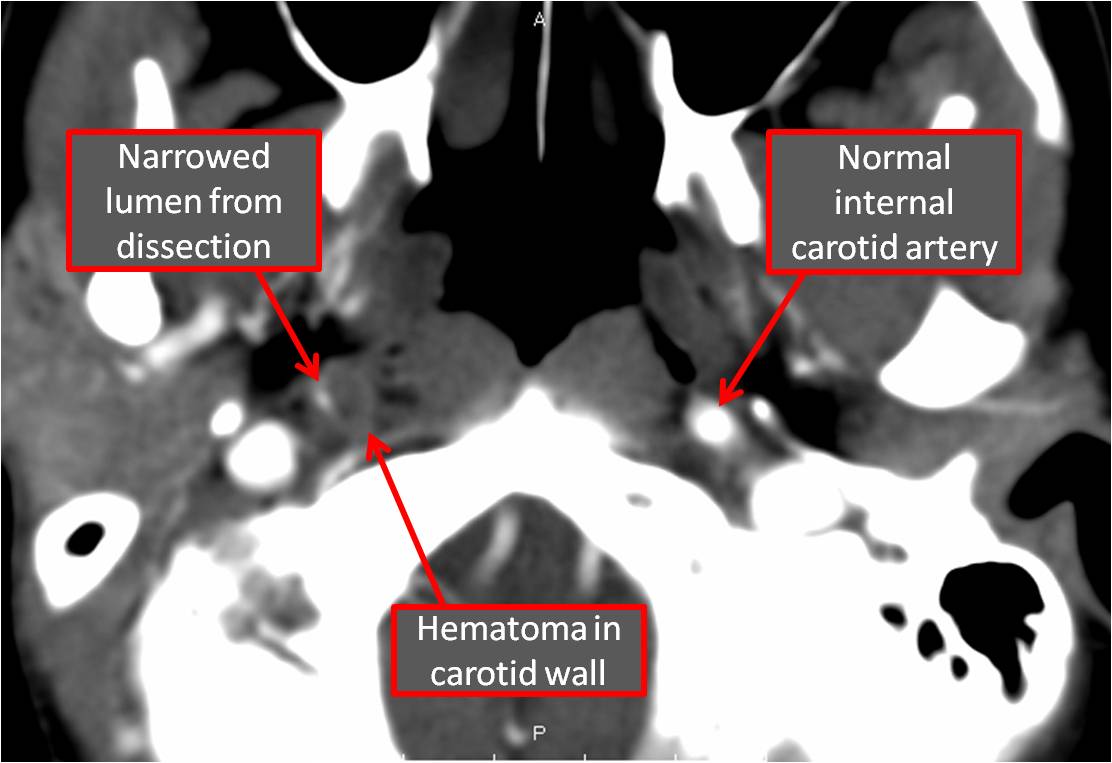
cervical artery dissection: quick review
--first consult call to Neurologists (less commonly Vascular Surgeons)
--Vascular imaging is a must, but CTA is more sensitive than MRA.
--To catch on MRI, specific sequences are required so check with your Neurologist/Radiologist to figure out which.
--Dissections that extend intracranially have a high incidence of forming SAH, especially when heparin is started, thus making heparin have higher mortality than anti-platelet drugs.
--Extracranial dissections are usually treated with antiplatelet drugs and anticoagulation.

Submitted by T. Boyd.
Reference(s): Shea et al. Carotid and Vertebral Artery Dissections in the Emergency Department. Emergency Medicine Practice.14;4. April 2012; picture
Tuesday, May 22, 2012
possible open joint: how much do I infuse?

--patient arrives with wound around the knee
--want to inject saline in the joint capsule to see if it is open (if it leaks)
--how much saline do I put in there?
Keese et al. The Accuracy of the Saline Load Test in the Diagnosis of Traumatic Knee Arthrotomies. J. Orthop Trauma. 21;7. Aug 2007.
--study of 30 patients undergoing arthroscopy
--after arthroscopy hole was made each knee was injected with saline and measure how much it took until extravasation was seen.
--50ml of saline gave 46% sensitivity
--194ml of saline gave 95% sensitivity.
FOOD FOR THOUGHT:
--standard 50ml injection not great sensitivity in this small study
--200cc NS seemed to do the trick
Submitted by T. Boyd.
Reference(s): article, picture
Thursday, May 17, 2012
d-dimer and aortic dissection
RAGING HYPOTHETICAL:
 --your patient arrives complaining of severe chest pain radiating to the back
--your patient arrives complaining of severe chest pain radiating to the back
--you fear aortic dissection
--you've heard about this d-dimer thing...but is it ready for prime-time?
HIGH IN PE/DISSECTION, NOT SO MUCH IN MI: (PMID: 21478122)
--purpose of this research was to define the D-dimer value for discrimination between AAD, PE and AMI.
--consecutive series of 35 AAD, 22 PE and 206 AMI patients
--D-dimer values of patients with AAD (32.9 ± 66.7 g/ml, p<0.001) and PE (28.5 ± 23.6 g/ ml, p<0.001) were significantly higher than those of AMI patients (2.1 ± 3.7 g/ml).
--A cutoff value of 5.0 g/ ml was effective in distinguishing AAD and PE from AMI, with a sensitivity of 68% and a specificity of 90% (ok, but not great)
GOOD SENSITIVITY IS PROMISING... (PMID: 21296332)
--Review and meta-analysis to examine use of d-dimer as screening tool for aortic dissection.
--A value of 500 ng/ml was defined as the threshold for a positive plasma DD finding because it is widely used for ruling out pulmonary emboli.
--Identified 7 studies involving 298 subjects with aortic dissection and 436 without.
--When data were pooled across studies:
NOT QUITE READY? (PMID: 21546117)
--There is inadequate evidence to support the use of D-dimer to exclude acute aortic dissection.
--registry data reported by Suzuki et al provide the most valid estimates for D-dimer sensitivity and specificity; however, the relatively small sample size (N=220) resulted in imprecise estimates, with a lower limit of the 95% confidence interval (CI) of 0.90 for sensitivity and 0.38 for specificity.
--A conservative estimate based on these results indicates that the negative likelihood ratio for D-dimer is approximately 0.2 and the positive likelihood ratio is 1.5. If these approximations are validated in a larger prospective study, a positive D-dimer result would have no value in clinical decisionmaking, but a negative D-dimer result may decrease the probability of aortic dissection to a moderate degree.
--However, to rule out aortic dissection with a negative D-dimer result, the pretest probability would have to be very low.
--Unfortunately, unlike pulmonary embolism or acute myocardial infarction, there are no validated clinical prediction rules to aid clinicians with establishing a pretest probability of aortic dissection.
Submitted by J. Gullo.
Reference(s): PMID: 21478122; PMID: 21296332; PMID: 21546117; picture

--you fear aortic dissection
--you've heard about this d-dimer thing...but is it ready for prime-time?
HIGH IN PE/DISSECTION, NOT SO MUCH IN MI: (PMID: 21478122)
--purpose of this research was to define the D-dimer value for discrimination between AAD, PE and AMI.
--consecutive series of 35 AAD, 22 PE and 206 AMI patients
--D-dimer values of patients with AAD (32.9 ± 66.7 g/ml, p<0.001) and PE (28.5 ± 23.6 g/ ml, p<0.001) were significantly higher than those of AMI patients (2.1 ± 3.7 g/ml).
--A cutoff value of 5.0 g/ ml was effective in distinguishing AAD and PE from AMI, with a sensitivity of 68% and a specificity of 90% (ok, but not great)
GOOD SENSITIVITY IS PROMISING... (PMID: 21296332)
--Review and meta-analysis to examine use of d-dimer as screening tool for aortic dissection.
--A value of 500 ng/ml was defined as the threshold for a positive plasma DD finding because it is widely used for ruling out pulmonary emboli.
--Identified 7 studies involving 298 subjects with aortic dissection and 436 without.
--When data were pooled across studies:
- sensitivity high (0.97, 95% confidence interval [CI] 0.94 to 0.99)
- negative predictive value high (0.96, 95% CI 0.93 to 0.98)
- specificity low (0.56, 95% CI 0.51 to 0.60)
- positive predictive value low (0.60, 95% CI 0.55 to 0.66)
NOT QUITE READY? (PMID: 21546117)
--There is inadequate evidence to support the use of D-dimer to exclude acute aortic dissection.
--registry data reported by Suzuki et al provide the most valid estimates for D-dimer sensitivity and specificity; however, the relatively small sample size (N=220) resulted in imprecise estimates, with a lower limit of the 95% confidence interval (CI) of 0.90 for sensitivity and 0.38 for specificity.
--A conservative estimate based on these results indicates that the negative likelihood ratio for D-dimer is approximately 0.2 and the positive likelihood ratio is 1.5. If these approximations are validated in a larger prospective study, a positive D-dimer result would have no value in clinical decisionmaking, but a negative D-dimer result may decrease the probability of aortic dissection to a moderate degree.
--However, to rule out aortic dissection with a negative D-dimer result, the pretest probability would have to be very low.
--Unfortunately, unlike pulmonary embolism or acute myocardial infarction, there are no validated clinical prediction rules to aid clinicians with establishing a pretest probability of aortic dissection.
BOTTOM LINE:
--studies used d-dimer cutoff of 500ng/ml
--high (but not perfect) sensitivity (90+%), low specificity
--potentially useful with patients with low pretest probability for aortic dissection
--since no validated prediction rules (like Wells/PERC for PE) for dissection, not quite ready for primetime
Submitted by J. Gullo.
Reference(s): PMID: 21478122; PMID: 21296332; PMID: 21546117; picture
Wednesday, May 16, 2012
fallopian tube torsion
WHAT IS
FALLOPIAN TUBE TORSION?

Twisting of
the fallopian tube on itself -- similar to closed loop bowel obstruction
Ovarian torsion is
more of an end tube twist, Fallopian tube torsion is proximal to ovarian
torsion
Much more rare cause of LQ abd pain/pelvic
pain than ovarian torsion
Prevalence:
one in 1.5 million women
Population at risk: pre-menopausal
women, 80% are <50 yo
Risk factors: Most commonly benign etiology (89%)
Intrinsic factors: long mesosalpinx, tortuous
dilated tube (hydro- or hemato-salpinx), tubal mass, tubal ligation, PID,
abnormal peristalsis/periovulatory spasm
Extrinsic factors: adhesions, adnexal venous congestion,
adjacent ovarian or paraovarian masses, uterine masses, gravid uterus,
trauma, sudden body position changes (Sellheim theory)
Proposed
mechanism: Mechanical obstruction of
adnexal veins/lymphatics --> pelvic congestion/edema --> enlargement
of fimbrial end --> partial/complete torsion of tube
Since vascular supply to adnexa comes from ovarian
+ uterine vessels --> can get isolated tubal necrosis w/o ovarian
vascular compromise
DDx: ovarian
torsion, ruptured ovarian cyst, PID, ectopic, appy, urolithiasis, cystitis,
SBO/perf
Difficult
diagnosis -- non-specific
findings, pain is only universal feature
Clinical
presentation
Sudden onset lower quadrant abdominal pain / pelvic pain
May be more intermittent than ovarian torsion (53% had previous
attacks of undx’d abd pain)
Slightly
more common on the right (3:2 R:L)
Labs: Leukocytosis
is mild, and late finding (>24 hrs after onset) -- tube likely unsalvageable
Ultrasound
findings
Normal ovaries + uterus with normal blood flow
Free pelvic fluid
Dilated adnexal tubular structure that flares at one end,
with thickened echogenic walls, suspicious for hydrosalpinx
A beaked, tapering
appearance of the tube, with its vertex pointing toward the affected adnexa
Internal
debris/convoluted echogenic mass, which may represent thickened torsed tube
Difficult to
visualize vascular compromise of tubal wall
CT
findings
Adnexal mass, twisted appearance to fallopian tube, dilated
tube >15 mm, thickened enhancing tubal wall, luminal attenuation >50 H
c/w hemorrhage
Free pelvic fluid,
peritubular fat stranding, enhancement + thickening of broad ligament, regional
ileus
Treatment
options
Surgical detorsion, salpingotomy
Salpingectomy
frequently performed 2/2 irreversible damage
Submitted by S. Eucker .
Reference(s): Gross, M et al, “Isolated Fallopian Tube
Torsion: A Rare Twist on a Common Theme”, AJR 2005; 185: 1590-1592. (Also the reference for the
images); Ho, P et al, “Isolated Torsion Of The Fallopian Tube: A Rare Diagnosis In An Adolescent Without Sexual Experience” Taiwan Normal
Fallopian Tube in a Premenarcheal Girl: A Case Report”, J Pediatr Surg 1990; 25(6):685-686.
Thursday, May 10, 2012
Kanavel signs for flexor tenosynovitis

--Kanavel signs for flexor tenosynovitis
- pain on passive extension (early finding)
- finger held in flexion
- uniform swelling of finger
- tenderness to percussion along flexor tendon sheath (late finding)
HOW GOOD IS OUR H&P?
--study of 75 patients with flexor tenosynovitis
--incidence of H&P findings
- fusiform swelling (97%)
- pain on passive extension (72%)
- semiflexed posture (69%)
- subcutaneous purulence (68%)
- tenderness along flexor sheath (64%)
- elevated WBC (59%)
- diabetes mellitus (35%)
- skin necrosis (23%)
- fever (17%)
--overall, the 4 signs aren't perfect, but are there individually in at least 2/3rds of patients
--hard to find data on sensitivity/specificity of these signs combined on brief pubmed biopsy
--IV antibiotics: staph and strep coverage, think pasturella for bite-associated infections
--surgery: consult your hand surgeon ASAP
Kanavel signs for flexor tenosynovitis (REVISITED)
- pain on passive extension (early finding)
- finger held in flexion
- uniform swelling of finger
- tenderness to percussion along flexor tendon sheath (late finding)
Reference(s): uptodate.com: infectious tenosynovitis; study; picture.
Wednesday, May 9, 2012
to CT or not CT?: Canadian CT Head Rule & New Orleans Criteria
CT or NOT?
 --Papa et al. study looked at both decision rules (link below)
--Papa et al. study looked at both decision rules (link below)
 --Papa et al. study looked at both decision rules (link below)
--Papa et al. study looked at both decision rules (link below)
--314 patients (73%) had a GCS of 15
--22 of the 314 (7%) had evidence of a traumatic intracranial lesion on CT
--3 of 314 (1.0%) required neurosurgical intervention
NEW ORLEANS CRITERIA (if ANY of these are true, then do a CT ):
- headache
- vomiting
- age > 60 years
- drug or alcohol intoxication
- deficits in short-term memory
- evidence of trauma above the clavicles
- seizure
CANADIAN CT HEAD RULES (if ANY of these are true, then do a CT):
- GCS < 13
- failure to reach GCS of 15 within 2 h
- suspected open skull fracture
- any sign of basal skull fracture
- vomiting >2 episodes
- age >65 years
- amnesia before impact >30 min
- dangerous mechanism of injury (pedestrian struck by car, ejection from MVC, fall > 3 feet or > 5 stairs)
--NOC and CCHR both had 100% sensitivity (95% confidence interval [CI] = 82% to 100%)
--CCHR was more specific (36.3% specificity) for detecting any traumatic intracranial lesion on CT vs. NOC (10.2% specificity)
Reference(s): study; mdcalc: canadian; mdcalc: new orleans; picture
Tuesday, May 8, 2012
stress dose steroids

--septic patient
--poured in lots of fluid, still hypotensive
--dripping in lots of pressors, still hypotensive
--um, what now?
POSSIBLE OPTION: STEROIDS (quick hits)
--'stress dose' steroids have been used for fluid/pressor unresponsive patients in septic shock
--hydrocortisone 50mg IV q6h, or 100mg IV bolus + drip (adults)
--not highly recommended in kids, unless known adrenal insufficiency
--rule of thumb stress dose for those on chronic steroids: 2-3x normal daily dose
--seems to have quicker resolution of shock, but not much mortality benefit
--slow taper later (thanks for taking care of this, ICU colleagues)
Reference(s): surviving sepsis recs, meta-analysis, uptodate.com: Hydrocortisone (systemic): Drug information, Corticosteroid therapy in septic shock, picture
{kind=link}
Monday, May 7, 2012
epileptic vs. non-epileptic seizure: what are the signs?
WHAT ARE THE SIGNS?
 --review by Avbersek & Sisodiya in J Neurol Neurosurg Psychiatry (link below)
--review by Avbersek & Sisodiya in J Neurol Neurosurg Psychiatry (link below)
--looked at 34 studies
--tried to tease out what signs distinguish epileptic vs. non-epileptic seizure
WHAT DID THEY FIND?
--signs that favor psychogenic non-epileptic seizures (specificity)
--signs that favor epileptic seizures (specificity)
--the sensitivities for all of these signs were horrible, so can't use them to rule anything out
--sometimes excluded frontal lobe partial seizures
--insufficient evidence: gradual onset, flailing/thrasing, opisthotonus, tongue biting, urinary incontinence
Reference(s): review article, picture

--looked at 34 studies
--tried to tease out what signs distinguish epileptic vs. non-epileptic seizure
WHAT DID THEY FIND?
--signs that favor psychogenic non-epileptic seizures (specificity)
- fluctuating course (96%)
- asynchronous movements (93-96%)
- pelvic thrusting (96-100%)
- side-to-side head/body movement (96-100%)
- closed eyes (74-100%)
- ictal crying (100%)
- memory recall (96%)
--signs that favor epileptic seizures (specificity)
- occurance from sleep (100%)
- post-ictal confusion (88%)
- stertorous (snoring) breathing (100%)
--the sensitivities for all of these signs were horrible, so can't use them to rule anything out
--sometimes excluded frontal lobe partial seizures
--insufficient evidence: gradual onset, flailing/thrasing, opisthotonus, tongue biting, urinary incontinence
Reference(s): review article, picture
Thursday, April 26, 2012
Spontaneous Cervical and Intracranial Arterial Dissections

Background
-Arterial dissections can cause stroke in both young in old populations, and is the most common cause of stroke in the young
-Extracranial dissection is more common than intracranial dissection
-Stroke is generally caused by either diminished blood flow from intraluminal thrombus or embolized clot
Pathogenesis (stick with it)
-Dissection are believed to begin with a tear in the media of the vessel wall, leading to bleeding in the wall itself
-partially coagulated intramural blood can enter the lumen which activates platelets and
the coagulation cascade leading to intraluminal thrombus.
-Intramural blood can accumulate leading to compression of the lumen
Risk Factors
-Connective tissue and vascular disorders are thought to be main risk factors:
(e.g. Ehlers-Danlos Syndrome (type IV), Marfan Syndrome, Polycystic kidney disease, cystic medial necrosis, Fibromuscular dysplasia)
-many are caused by trauma
Diagnosis
-based on radiologic criteria taken from the Strategies Against Stroke Study for Young Adults in Japan (SASSY) using CTA or MRI/MRA
-Primary rules are based on finding an intimal flap or double lumen on Angiogram or MRI/MRA, or repeated non-specific findings associated with dissection on multiple studies.
Symptoms
-Head or neck pain
-Horner Syndrome - occurs when the sympathetic fibers on the ICA are stretched. It is usually just partial with ptosis and miosis but no anhidrosis.
Difference between Carotid and Vertebral Dissections
-Transient monocular blindness occurred only with internal carotid dissection
-Ischemic stroke is more common in vertebral dissections
-Neck pain and recent minor cervical trauma are more common in vertebral dissections
-Proportion of men and a recent infection are more common in ICA
Treatment
-Antithrombotic therapy (antiplatelet or anticoagulation) is the primary initial treatment for ischemic stroke and TIA caused by arterial dissection
-For intracranial dissection, antiplatelet therapy is often the treatment of choice
-For extracranial dissection, anticoagulation initially followed by 6 months of warfarin therapy as opposed to antiplatet therapy is often chosen
-Endovascular and surgical therapy are generally only reserved for recurrent ischemic events
BOTTOM LINE:
-arterial dissection is more common cause of stroke in the young
-extracranial (vertebral, carotid) more common than intracranial dissection
-sx: headache, neck pain, stroke-like symptoms, Horner's syndrome (for ICA)
-risk factors: connective tissue disorders, trauma
-dx: angiography, MRI/MRA
-tx: antithrombotics/anticoagulation (aspirin, heparin, coumadin, etc.); surgical/endovascular for recurrent events
Submitted by J. Grover.
Reference(s): Caplan, LR and Biousse V. “Cervicocranial Artery Dissections.” J Neuro-Opthalmol. 2004; 24:299-305. Maruyama, H et al. “Spontaneous Cervicocephalic Arterial Dissection with Headache and Neck Pain as the Only Symptom.” J Headache Pain (2012) 13: 247-253. “Spontaneous Cerebral and Cervical Artery Dissection: Treatment and Prognosis”. Uptodate. “Spontaneous Cerebral and Cervical Artery Dissection: Clinical Features and Diagnosis”. Uptodate., picture
Tuesday, April 24, 2012
octreotide in sulfonylurea overdose
BASIC IDEA:
--Octreotide inhibits the secretion of several neuropeptides, including insulin
--if someone overdoses on a sulfonylurea (e.g. glipizide), would giving octreotide help reduce the hypoglycemia problem?
(straight to the) BOTTOM LINE:
--limited studies out there, but reviews tend to say the same thing...
--octreotide is probably safe and beneficial in sulfonylurea overdose/hypoglycemia
Reference(s): http://www.ncbi.nlm.nih.gov/pubmed/17764782 , http://www.ncbi.nlm.nih.gov/pubmed/16356235, http://www.ncbi.nlm.nih.gov/pubmed/17652687, http://www.ncbi.nlm.nih.gov/pubmed/20352540
--Octreotide inhibits the secretion of several neuropeptides, including insulin
--if someone overdoses on a sulfonylurea (e.g. glipizide), would giving octreotide help reduce the hypoglycemia problem?
(straight to the) BOTTOM LINE:
--limited studies out there, but reviews tend to say the same thing...
--octreotide is probably safe and beneficial in sulfonylurea overdose/hypoglycemia
Reference(s): http://www.ncbi.nlm.nih.gov/pubmed/17764782 , http://www.ncbi.nlm.nih.gov/pubmed/16356235, http://www.ncbi.nlm.nih.gov/pubmed/17652687, http://www.ncbi.nlm.nih.gov/pubmed/20352540
Thursday, April 19, 2012
fat pad on x-ray
WHAT IS THE FAT PAD?
--might be only subtle sign of a fracture on x-ray
--broken bones leak fat & blood, which also moves existing soft tissue


COOL TRICK:
--courtesy of EM News article (check out the pic on their website)
--if you're aspirating a joint (e.g. knee effusion), and you aspirate blood, take a look under a light, look for the sheen of fat on top (suggests fracture)
 --might want to get a CT or MRI next, if those x-rays were negative
--might want to get a CT or MRI next, if those x-rays were negative
Reference(s): EM News article with picture, x-ray, diagram, oil&water
--might be only subtle sign of a fracture on x-ray
--broken bones leak fat & blood, which also moves existing soft tissue


COOL TRICK:
--courtesy of EM News article (check out the pic on their website)
--if you're aspirating a joint (e.g. knee effusion), and you aspirate blood, take a look under a light, look for the sheen of fat on top (suggests fracture)

Reference(s): EM News article with picture, x-ray, diagram, oil&water
Wednesday, April 18, 2012
hydrofloric acid burns

--one of the strongest inorganic acids
--can cause significant systemic toxicity due to fluoride poisoning.
--is used mainly for industrial purposes (eg, glass etching, metal cleaning, electronics manufacturing)--may be found in home rust removers.
TREATMENT TOOLBOX:
--can be soaked in magnesium hydroxide containing solutions (e.g. Mylanta) or soaked in ice water to help decrease the amount of absorption.
--decontaminate appropriately and wash with water.
--apply 2.5% calcium gluconate gel to burn (10% Ca Gluconate solution in 3 times the volume of KY gel) and place hand into latex glove.
--if pain persists >30 minutes and not on fingers, infiltrate margins of burn with 10% calcium gluconate solution.
--if severe burns, can inject 10ml of 10% Ca gluconate in 40ml of D5 intra-arterially over 4 hours.
--repeat as necessary. For oral, ocular, or inhalation burns, calcium will also have to be given in different concentrations.
--Consult Toxicology.
--Treat pain with opioids.
Submitted by T. Boyd.
Reference(s): http://emedicine.medscape.com/article/773304-treatment, picture
Subscribe to:
Comments (Atom)